
How Breastmilk is Made
I don't understand why lactation should be a mystery to so many people. We are taught how other systems in our bodies work, and all about the reproductive system, at school. There might be a paragraph or two describing the “benefits” of breastfeeding and maybe even a diagram of the breast anatomy. High school students studying Health and Human Development might get a bit more detail but most people leave school without knowing much, if anything, about how humans make milk.

Antenatal educations tends to focus mostly on the birth
People who attend hospital antenatal classes are going to learn pretty much the same content as their school biology classes addressed, with a bit more information on sore nipples, mastitis and how to position a baby to latch. But the content about how breasts make milk is still pretty basic. Breastfeeding classes offered by organisations like the Australian Breastfeeding Association and private midwives or IBCLC lactation consultants will provide more detail.
Yet when it comes to supporting new mothers who are learning to breastfeed, often the most basic information is missing from their knowledge and their concerns are eased by finding out how their body works to supply milk for their baby.
So let's look at lactation in some more detail.
On the Outside
Breasts typically come in pairs but rarely a matching set. Most people have one larger than the other which can even be a cup-sized difference in bras. The breast skin near the nipple changes in appearance, typically darker than surrounding skin and darkening further in pregnancy. However, the degree of colour difference varies from barely anything to dramatic and all are normal. This area is known as the areola. There are usually small bumps on the skin of the areola closer to the nipple. These Montgomery Glands secrete natural oils to moisturise the skin, meaning creams and balms are unnecessary.

The nipple is often seen as the star of the show and a lot of attention is paid to their appearance. Just like breasts, no two nipples are the same. They can be long or short, wide or narrow, large or small, flat, erect or inverted. Some people even have one or more extras!. These bonus nipples might have some breast tissue behind them or just be darker spots on the skin.
Babies BREASTfeed by drawing the nipple deeply into the mouth and using their tongue and jaw to remove milk. The nipple is an aid to babies attaching and contains duct openings where the milk comes out. (We’ll come back to them later)
Nipples, like other parts of the body including the mouth, have incredibly sensitive skin which damages easily but heals rapidly. The sensitive skin is important as this is how your baby communicates with the breast to release milk. Even brushing against the nipple or the light touch of clothing can trigger that release, so sensitive are the nerves in that area. Touch also causes the nipple to become erect making it easier for the baby’s mouth to find. Inverted or flat nipples still do the job but young babies can need help in the early days.
On the Inside
One of the very first signs of puberty can be the first growth of breast tissue behind the nipple of girls as young as 8-10 years. Changing hormones switch on the development of mammary glands. Over the next several years, the breasts respond to the hormonal messages and set up the system for future lactation. Most girls complete this development in their mid-teens. Occasionally, the development of breast tissue is interrupted or affected by other factors and a woman may have a range of conditions named collectively as Insufficient Glandular Tissue. Depending on the degree of variation this might mean low to no lactation occurs during the postnatal period. This can be very obvious from appearance but the breasts can also appear typical but be functionally impacted internally. A doctor or IBCLC lactation consultant can identify potential issues during a routine examination in pregnancy or it might be recognised in the postnatal period when breasts are not producing milk as expected.

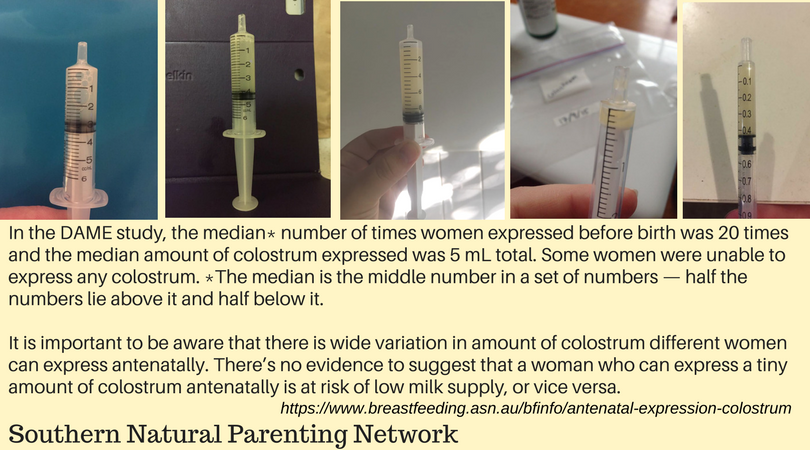
When typical development has occurred during puberty, the next update happens soon after a first pregnancy is conceived. Tender nipples and swollen breasts can be part of some women's menstrual cycle and are relieved by the onset of bleeding. In early pregnancy, without that change of hormones, this discomfort can continue as breasts set up the infrastructure to produce milk. So early is this development that some women are excreting small amounts of colostrum at the end of the first trimester and may have gone up a bra size or more. Other women have a more subtle experience of this stage and might not leak any colostrum in pregnancy or notice breast growth. This is not uncommon but worth mentioning to your midwife or doctor. Later in the final weeks of pregnancy some women can collect expressed colostrum to store, however research has found not everyone can do so. This is not an indicator of successful milk production or breastfeeding ability but just normal variation between people.
Until recently, our understanding of the internal anatomy of the breast was very different. Due to the diligent work of Australian researchers in Western Australia, utilising ultrasound technology in the late 90s and early 00s, we now know that earlier descriptions were flawed. Anatomy of the lactating human breast redefined with ultrasound imaging D. T. Ramsay, J. C. Kent, R. A. Hartmann, P. E. Hartmann

Many people assume the breast fills and empties like a bladder. However the mammary glands work more like sweat glands, releasing milk as needed. You don’t have to wait for them to refill and they are never actually empty. Indeed, research has also shown babies only take about 67% of available milk. Breastfeeding advisors are moving away from using terminology like “full”, “empty” or “drained” when describing the breast as these are not accurate.
By the time babies are born - even if very prematurely - the breasts are primed and ready to feed them. Regardless of a mother’s intention to breastfeed the system is established and waiting for the baby to arrive.
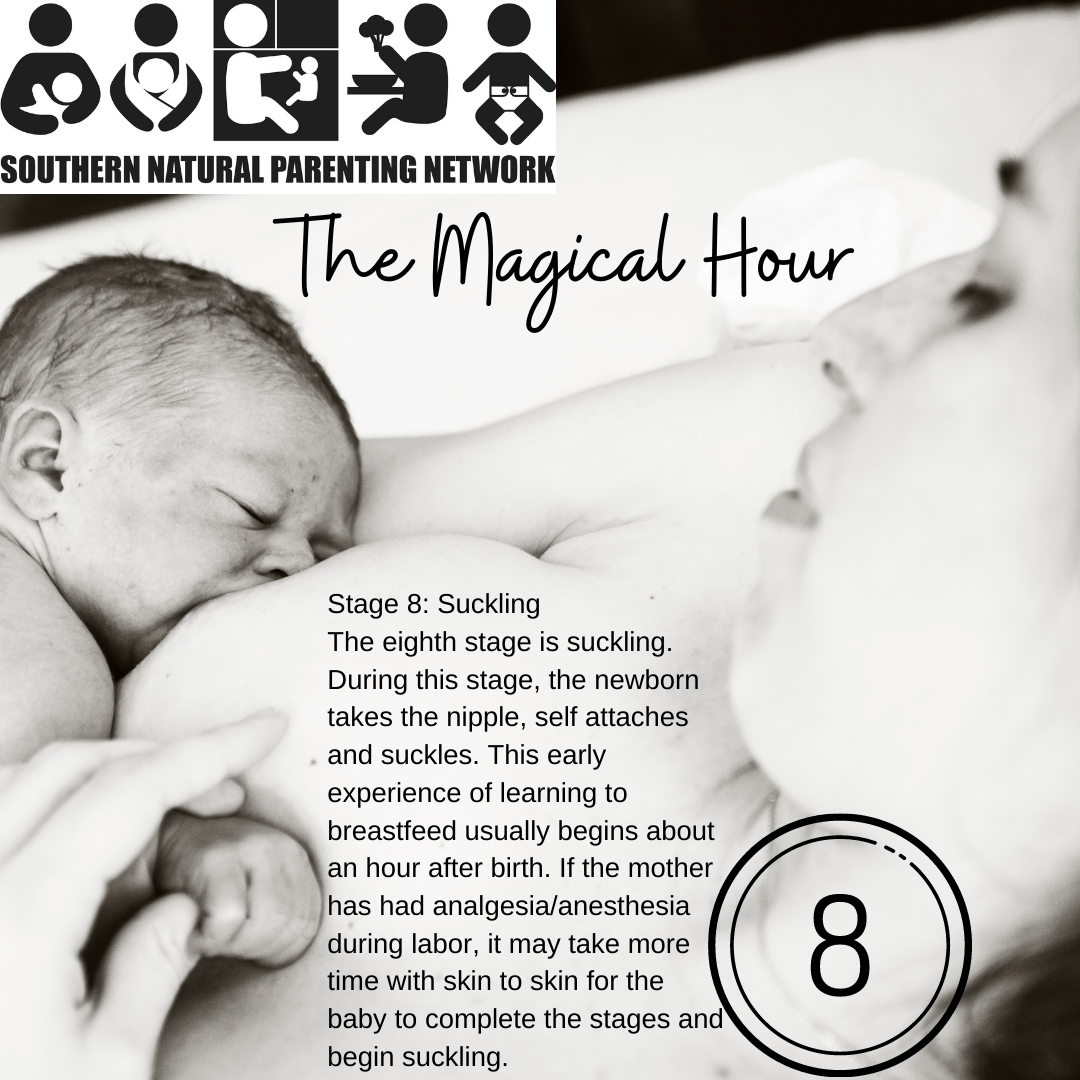
The Magical Hour
The birth of the baby is celebrated as the end of pregnancy but overlooked in its significance as the beginning of breastfeeding. Exiting the womb through vaginal childbirth, the infant simply pauses before beginning the next journey: from belly to breast.
The Breast Crawl is a natural consequence of birth. The infant will next travel up the mothers body to find the breasts, seek the nipple and attach. Unless the birth has included interventions, including some medications, the baby will do this independently, with minimal guidance from the mother and a hands-off approach from midwives. Where babies are born surgically or with other interventions, the process might be delayed but will still happen when the opportunity is given.
The Magical Hour is used to describe this series of nine stages babies progress through naturally:









When medical issues mean mother or baby are not able to initiate breastfeeding within the first hour, it is still important that the breasts receive the signal the baby is born. Hand expressing by or for the mother is important. Expressing this first milk if the baby does not go to the breast reduces the risk of formula supplementation during the hospital stay.

Switching Lactation On
You might be surprised that it isn’t the birth of the baby which signals to the body to to move to the next stage of lactation. It is actually the placenta exiting the womb and the sudden drop in the hormone progesterone after the birth which triggers the next stage.
The needs of the newborn baby in the first days after birth are met in several ways:
Colostrum is concentrated breastmilk high in protective factors which support the immature immune system, seeds the infant gut microbiome and provides energy.
Fluid absorbed in the womb over-hydrates the infant, so they do not need large volume feeds and can slowly expand the stomach. A healthy newborn is expected to lose 7% to 10% of the birth weight, mostly due to losing this extra fluid and utilising their brown fat stores as an energy source.
Brown fat stored during pregnancy provides additional energy to the baby and protects newborns against becoming too cold. Newborns can’t shiver, a response to warm the body, so they use this stored energy instead. These fat stores, predominantly around the shoulder blade area, protect the core from becoming too cold.
Babies arrive with a packed lunch and a water bottle: they don’t need large volumes of breastmilk - if they did, nature would provide that.


It is around 72 hours after delivery that breasts begin to produce milk differently. Having gently introduced the baby to feeding and digestion, now its time for lactogenisis: literally “the beginning of milk making”. I like to call it the “milk making marathon” because, suddenly, that sleepy newborn wakes up and demands milk. A lot.

Possibly the most intense stage of breastfeeding is the period when the baby instinctively seeks the breast frequently around the clock for around 24 hours. Giving frantic feeding cues and signaling distress, mothers should instinctively respond by offering the breast frequently. Together, baby and mother facilitate the frequent stimulation needed to transition the milk from colostrum to mature milk.
This process is threatened by interventions based on expectations of infant behaviour or weight during this time period. This include:
Restricting access to the breast based on time-based routines
Substituting dummies or bottles to meet the infant sucking demand instead of the breast.
Interpreting the frequent feeding as a sign of pain, hunger or ineffective technique.
Feeding the baby with infant formula supplements - top-ups - to lengthen the period between feeds and induce sleep.
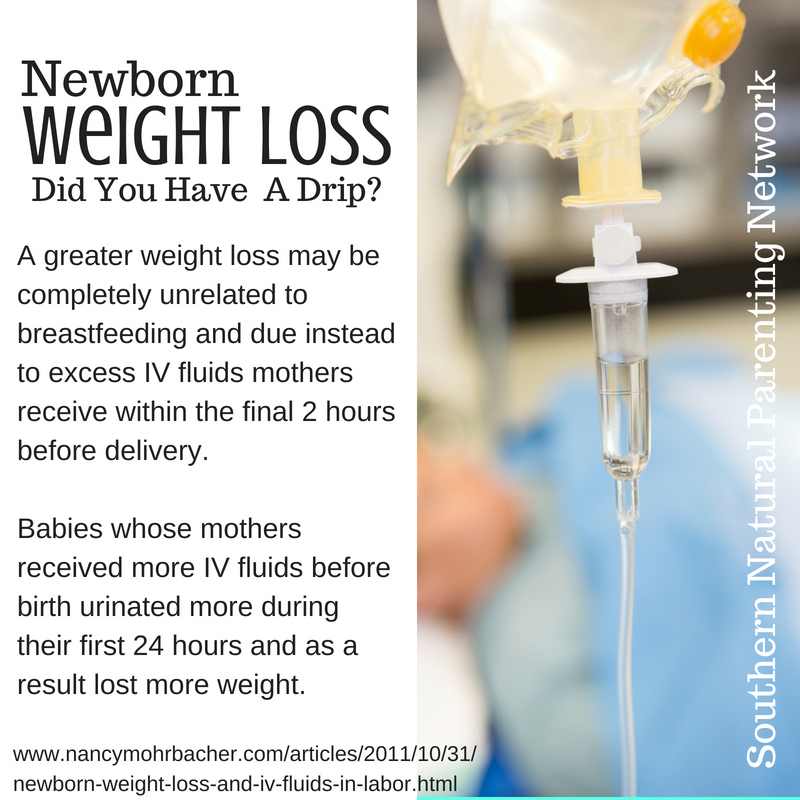
The timing of this natural process unfortunately clashes with the social requirement for mothers and babies to be discharged from hospital around about the same time after delivery. Just as mothers are preparing to leave hospital and the support system it provides, their baby begins feeding more, crying more and sleeping less. Routine weighing of babies before discharge has shifted in the timeline: when mothers stayed in hospital 7-10 days after vaginal delivery, their babies had begun to regain weight after the normal loss in the first week. Now, with just 24-48 hours stay, this weigh-in falls right at the time when babies have lost the most weight, prior to the volume of milk increasing and weight gain beginning. This slight change has seen an increase in concern about babies weight and the introduction of infant formula. Making matters worse, as birth interventions including induction and surgical delivery increase, more women receive intravenous (IV) fluids during labour and delivery: artificially increasing the infant birth weight and distorting actual weight loss.
When no interference occurs, this powerful cluster feeding sends clear messages to the breast and establishes the milk production.
Previously described as the milk “coming in” new terminology better describes this process. As we have seen, breastmilk - in the form of colostrum - is present in the breasts well-before the baby is born. What does happen is an increase in the volume of the milk as it begins the transition to the mature breast milk. The breasts become fuller and heavier when this occurs and frequent milk removal is needed to keep the balance right. Delaying breastfeeds, restricting time at the breast or sleepy babies who aren’t going to the breast often enough can mean the breast holds more milk and breasts can feel swollen and sore. Traditionally known as engorgement, blood and other fluids in the breast add to this uncomfortable fullness and the breast may become so swollen the baby struggles to latch on!
Feeding the baby at least every 2-3 hours day and night helps keep the breast tissue comfortable and helps balance the milk production with the baby’s needs. Avoid very long intervals between feeds by waking the baby if they sleep longer than 3-4 hours. This stage usually lasts around 24 hours and early and frequent feeding or expressing of milk from birth helps prevent discomfort.
The First Weeks
Frequent removal of milk signals to the breast to continue lactation. This is described as supply and demand. The more you remove (demand), the more you make (supply). Two hormones have critical roles in the feedback loop between baby and breast:
Oxytocin - stimulation of the nipple sends signals via the nervous system to a gland near the brain - the hypothalamus. Oxytocin release causes tiny muscles around each milk gland to tighten, causing milk to flow into the system of ducts for the baby to remove.
Prolactin - is also released into the bloodstream, signaling to the glands to increase milk production in response to milk removal.
Combined, we refer to this as the Let-down Reflex or Milk Ejection Reflex. Oxytocin is known as the hormone of love and as it floods the mother’s body, her bond with her baby is strengthed, motivating her to dedicate her time and energy to lactation.

The Let-down reflex occurs multiple times during a feed (or pumping session) but often it is most noticeable the first time. Some mothers don’t feel anything physically but notice the baby’s sucking and swallowing become deeper and more rhythmic. Others also experience sensations in one or both breasts, of tingling, heaviness or similar feelings. The resting breast responds to the let-down at the same time as the active breast and it might ooze, drip or spray milk for a moment or two. A very strong let-down reflex can send milk quickly out of the breast, overwhelming the baby as they struggle to keep up. Others get impatient as the let-down takes a little longer and they might fuss or protest until the milk flows. All are normal variations on this natural process and both mother and baby soon adjust to their experience.
The milk initially ejected from the breast quickly quenches baby’s thirst with its high water content and gradually increases in energy as the glandular issue steadily releases higher-fat milk into the mix. Sometimes you can even observe the different stages unblended when you express your breastmilk - white streaks not quite mixed with the blue-white early milk. By the time the baby has taken what they want from that side, the milk is rich and creamy and might ooze rather than drip when you are expressing. If you set this milk aside, you might later see it has separated into two layers: the fat content rises to the top and floats on top of the lower-fat milk below. Your grandparents might remember bottles of cows milk looked like this in their childhood, before homogenation processes were common. If you observed standing breastmilk expressed at different times of the day, you would see variations not only in volume but in the layers of creamy fat compared to the bulk of the milk. This is entirely normal and not something you are even aware of when direct feeding at the breast.
The fat content of breastmilk changes throughout the day. When breastfeeds are very close together - like we see in cluster feeding - the fat content remains high. As time passes between removals of milk (feeds or pumping sessions) the percentage of fat decreases as the milk glands draw it back in, ready to release next time the let-down reflex is triggered. A soft breast which you might think is “empty” is more likely to be holding a low volume of high calorie milk rich in fat. But that “full” feeling breast which has gone hours since the last feed will be full of lower-fat milk. This is why stretching out the time between breastfeeds cannot increase your milk supply: full breasts slow down production, while soft breasts speed it up. And if you want to increase your baby’s weight gains, frequent feeds allow hem to maximise that high-fat milk which is so important for growth.
That heavy full breast is signaling to the body to slow down breastmilk production by releasing a substance known as the Feedback Inhibitor in Lactation, or FIL. This effectively puts the brakes on to regulate the volume of milk being produced, as storage space can only hold so much! Without this, things could become very uncomfortable indeed! But the more often milk is removed from the breast, the lower the stored volume and the less FIL is released: putting the accelerator down on milk production.
Breasts are never empty. There is always more milk available - as much as one third of capacity. But babies are like the rest of us - they don’t like to work too hard! And that rich, creamy milk high in fat takes effort to remove when feeding - breast pumps can’t even get it all, with hand-expressing being more effective. A full, sleepy baby who is grazing the dessert table will often doze off to sleep at this point. A baby who is still hungry will reach a point of taking the easy option, come off the first breast and seek the second. The milk in the second breast already has a higher fat content from the let-down reflexes triggered on the first, so the baby will probably feed here for a shorter time. But during cluster feeds and during periods of rapid development, they might take their fill from the second breast as well and sometimes, come back to the first to top-up with that rich milk. Sometimes this is called “licking the plate” which is a great description, as babies growing rapidly take advantage of the way breasts produce milk.












Expressed breastmilk is a snapshot of the volume and appearance at the time of collection. The amount you can collect is NOT an indication of milk supply or production, simply the amount you could effectively remove by hand-expressing or using a breast pump. A well-attached baby will always be the most efficient way of removing milk from the breast. The volume of milk your breasts have the capacity to store at any one time is unique to you and the volume of milk produced by individual women varies significantly. As does the volume of milk taken by individual babies.
Over-production of Breastmilk
In the first stage of lactation the breasts respond to milk removal to establish supply and demand. The amount of milk the baby takes effectively programs the production , which is maintained once established. A modern issue is the use of breast pumps and milk collectors in addition to direct feeding in the early days. While these can be a useful tool in protecting the milk production while resolving feeding problems in the baby due to poor attachment, tongue ties, jaundice or other medical challenges, when used too enthusiastically they can create an artificial extra demand, leading to ongoing over-production of milk. Some parents, keen to include non-breastfeeding parents in feeding the baby or anticipating an early return to the paid workforce where paid parental leave is not available start expressing early and often and run into problems when their supply of frozen expressed breastmilk overtakes their freezer!
Where possible, avoid expressing for non-medical reasons in the first two weeks and then introduce it gradually. Milk collectors which suction onto the breast have become a problem for some women, as they routinely use them for what they believed to be passive milk collection. However the suction holding them in place can cause more milk to flow than would naturally leak in response the let-down reflex. Using these or a breast pump at most or all feeds basically tells the body you are feeding more than one baby and your milk production will use that feedback to establish your supply.

Too much of a good thing … be careful what you wish for!
Low Milk Supply
Where there are no physical variations in mothers (eg Insufficient Glandular Tissue) or baby (eg tongue tie) then milk production can be expected to establish in response to the newborn’s regular feeding. If a baby is feeding effectively - as often as they need, for as long as they need - supply will match demand.
Parental limits on frequency or length of feeds is a major cause of imbalance between supply and demand. Routines, schedules, dummies and sleep training all interfere with the natural feedback loop between baby and breast. The concept of “feeding too often” is out-dated and dangerous when it comes to breastfed babies. Breastfed babies will spend most of their waking hours feeding in the early months. This is not a problem to be solved.

When babies are not latching well, the amount of milk they remove is impacted. The milk is available but they are not efficiently feeding. This is usually due to poor attachment and likely the mother will also be experiencing nipple pain and damage.
However, while some supplies are low due to the above reasons, far more common is Perceived insufficient milk supply (PIMS). Sadly, this ranks as one of the most common reasons women stop breastfeeding. Their body is producing more than enough milk for their baby but they lack confidence because their expectations of breastfeeding aren’t in-line with their experience. The most common reasons given for believing their baby is not getting enough milk are:
Their baby feeds more frequently and for longer periods than they believe could be normal
Their baby sleeps for shorter periods and wakes more in the night than they believe could be normal
Overwhelmed parents seeking help from overwhelmed health professionals will often result in the baby being given expressed breastmilk and/or supplemental formula feeds, with mothers instructed to pump after every breastfeed. Triple Feeding is even more time-consuming than the original situation and parents are very likely to move to fully feeding their baby infant formula.
In a recent study in Western Australia, 44% of the mothers had a perception of insufficient milk supply within 3 weeks of birth. The most common reason for this perception was that their infant was not satisfied after breastfeeds.
Western society has unreasonable expectations based on decades of formula feeding culture in the mid to late 20th century. Sleep training advice to put babies to bed drowsy but awake; routines dictating the length and frequency of breastfeeds to the minute and poor understanding of typical infant behaviour and development are all causes of the unrealistic belief in babies spending large blocks of time asleep with short periods of feeding in-between, when the reality is much different.

The most vulnerable times during breastfeeding for mothers to doubt their milk supply are in the first week, around three weeks and around 6-12 weeks. These are stages of transition in milk production and significant changes occur. Parents have the right to know and be prepared for these shifts in lactation and be supported to continue frequent feeding through them.
Milk Supply Regulation: around 6 - 12 weeks, the training wheels come off!
The milk supply is locked-in and running like a well-oiled machine and now your baby receives the milk they need, when they need it. The breasts are no longer heavy and full-feeling before you feed and may feel soft and … empty. But nothing could be further from the truth. From now until weaning, the breast produces milk at a steady, reliable pace. Researchers have measured the volume of milk produced and the volume of milk taken in mothers and babies of babies aged one to six months and the results were surprising: the volume of milk changes little and remains consistently the same, with the baby varying only how often and when they access it. The variation between feed frequency is 8-12 times in 24 hours but some healthy and happy babies in the study went to the beast as many of 17 times in a day! They simply preferred little and often, while babies at the other end of the scale took large feeds as few as six times in 24 hours. All normal. And the average volume of milk still in the breast after a feed? 67%. Babies don’t drain or empty the breast. They feed until they are full. They actually come off the breast when one of the multiple let-downs or milk-ejections occur!
Breastmilk continues to meet the infant’s nutritional needs for at least six months and will meet the majority of their needs for 12 months. When family foods are introduced, only minimal extra nutrients are necessary - iron and zinc for example - and not significant extra calories or energy. What used to be called an “educational diet” in the second half year is about learning how to eat, not replacing breastmilk. And throughout the natural breastfeeding period of 3-4 years, with a minimum of 24 months, breastmilk provides essential nutrients, energy and immune support as well as components only found in human milk required for growing human brains and bodies. There is no upper limit to the importance of breastfeeding - every drop makes a difference.
Breastmilk has kept human infants alive for millions of years. It has not suddenly “failed” us in a matter of decades. Trust in breastfeeding has been undermined by aggressive marketing of infant formula in targeted campaigns intended to create doubt and mistrust of natural feeding. Very few women cannot produce breastmilk. Very few babies cannot take breastmilk. However, lack of education and support in the wider community is needed to give parents faith in the breasts to meet infant’s needs.
Australia and New Zealand, as well as countries like the US and UK can and must do more to protect breastfeeding for its important role in public health. Investing in breastfeeding education and support means less spent on the diseases in later life which are more common in adults who were formula-fed.

